|
Under 10 years
|
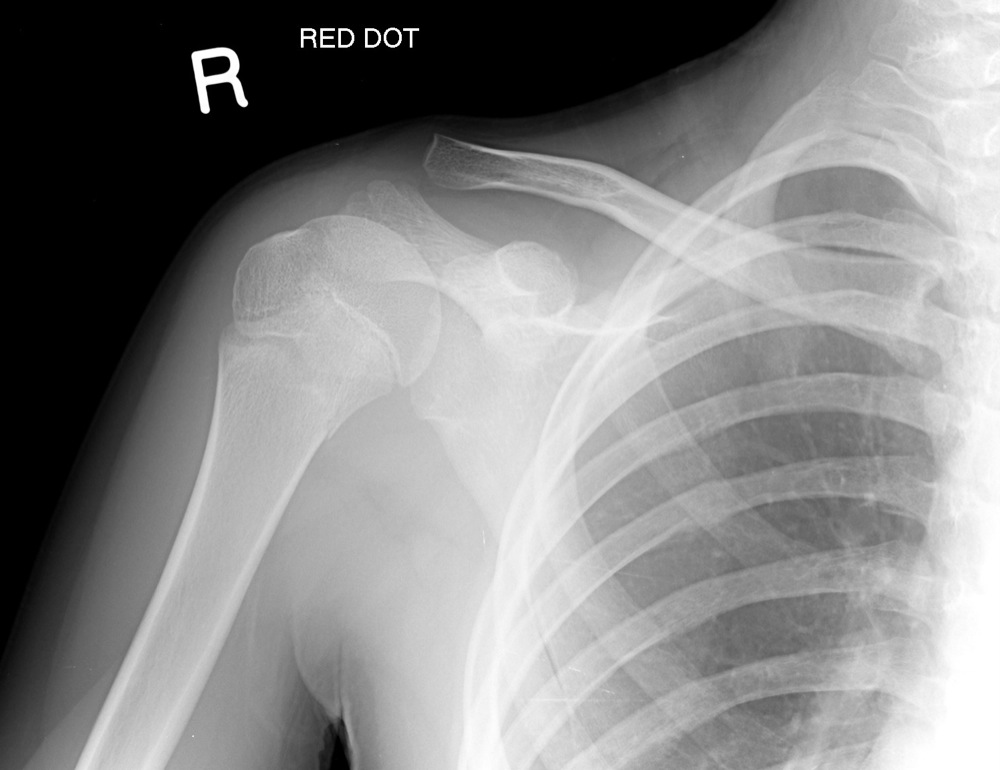
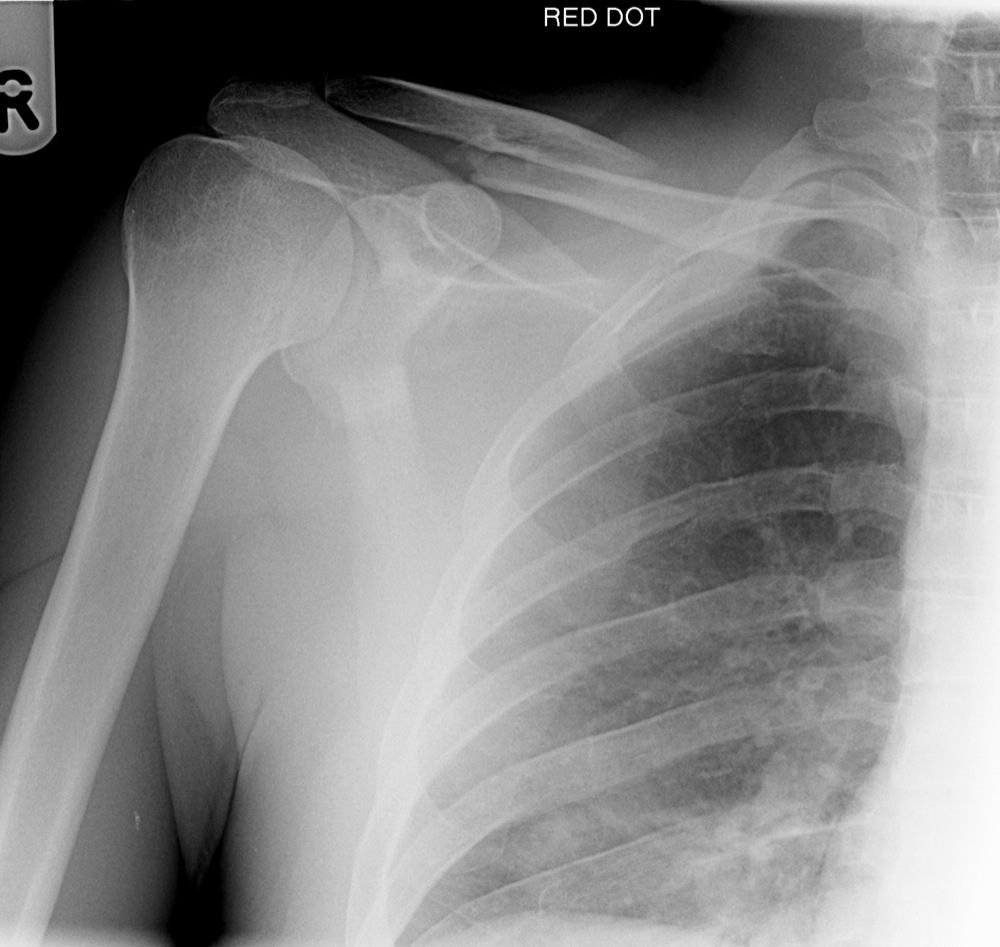
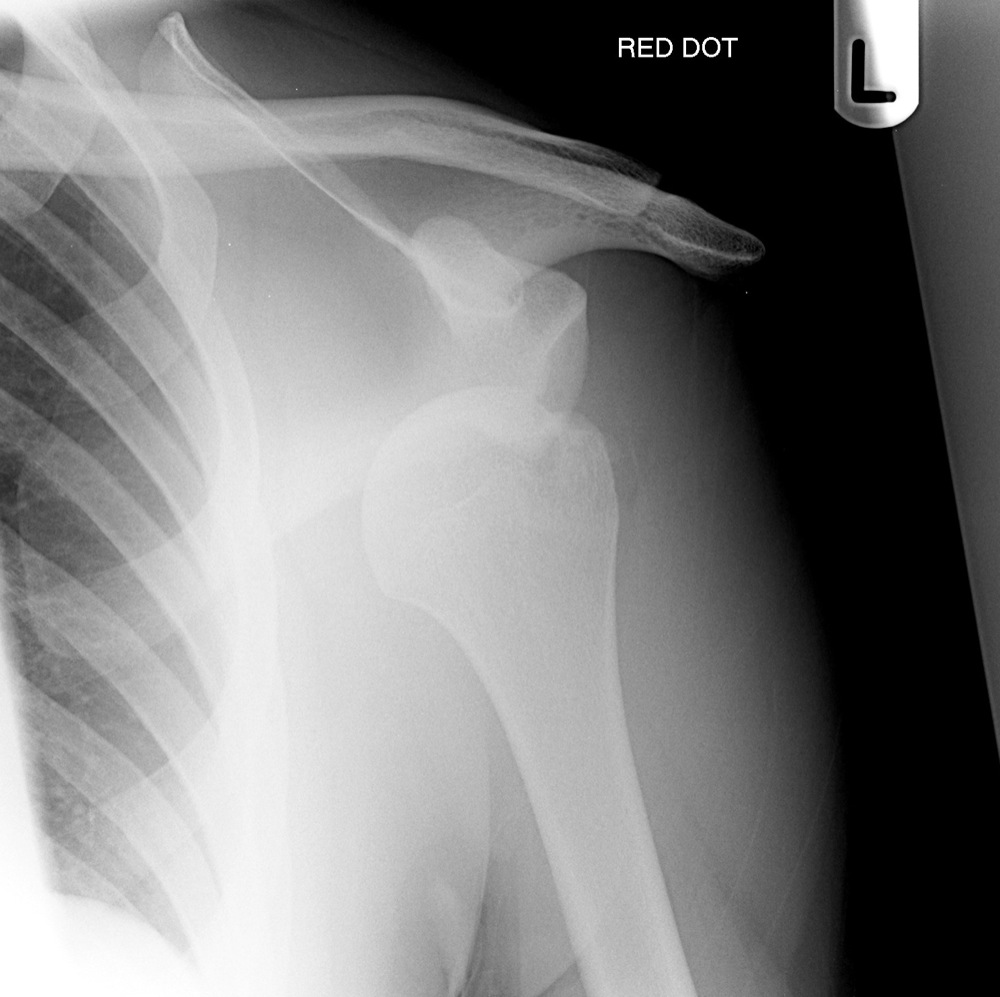
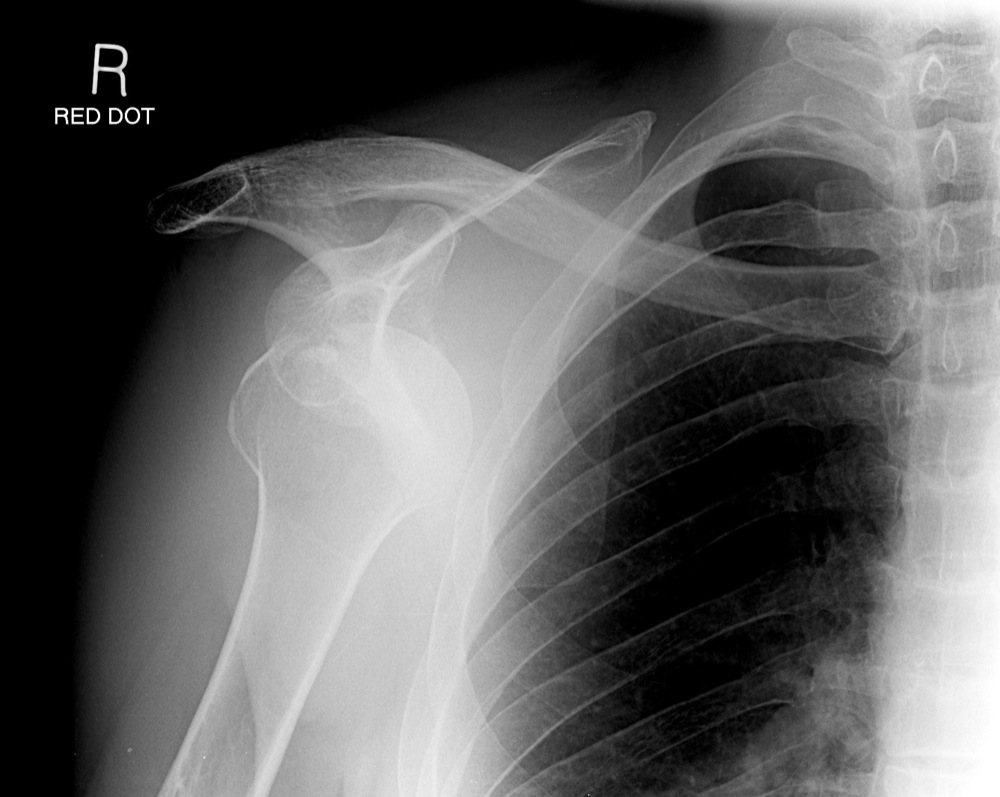
Fractured clavicle |
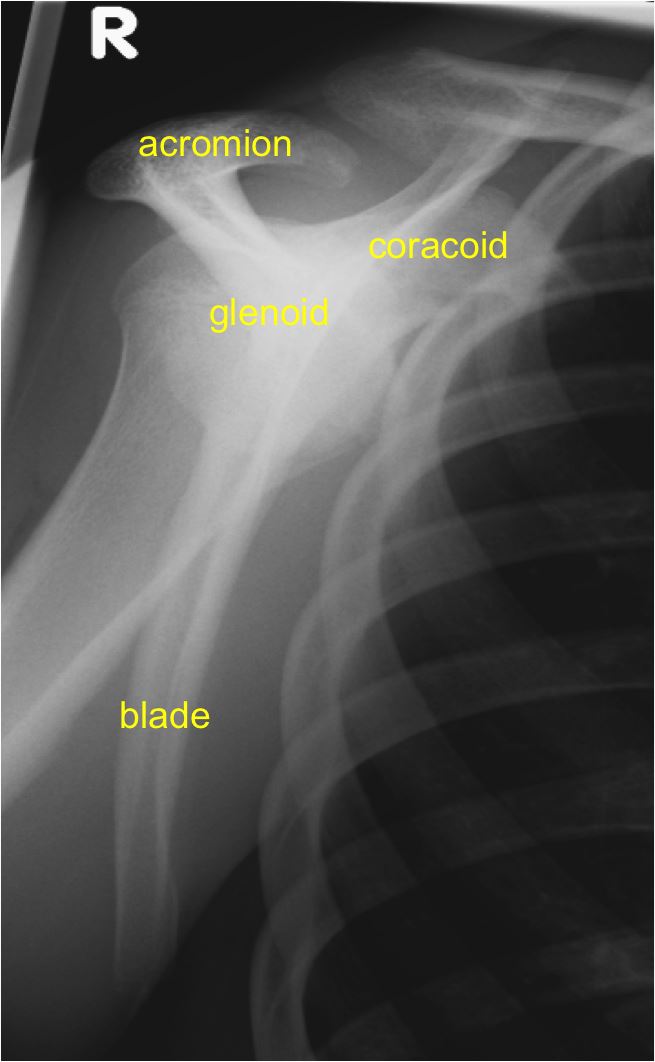
| 15-40 years | Acromioclavicular joint subluxation |
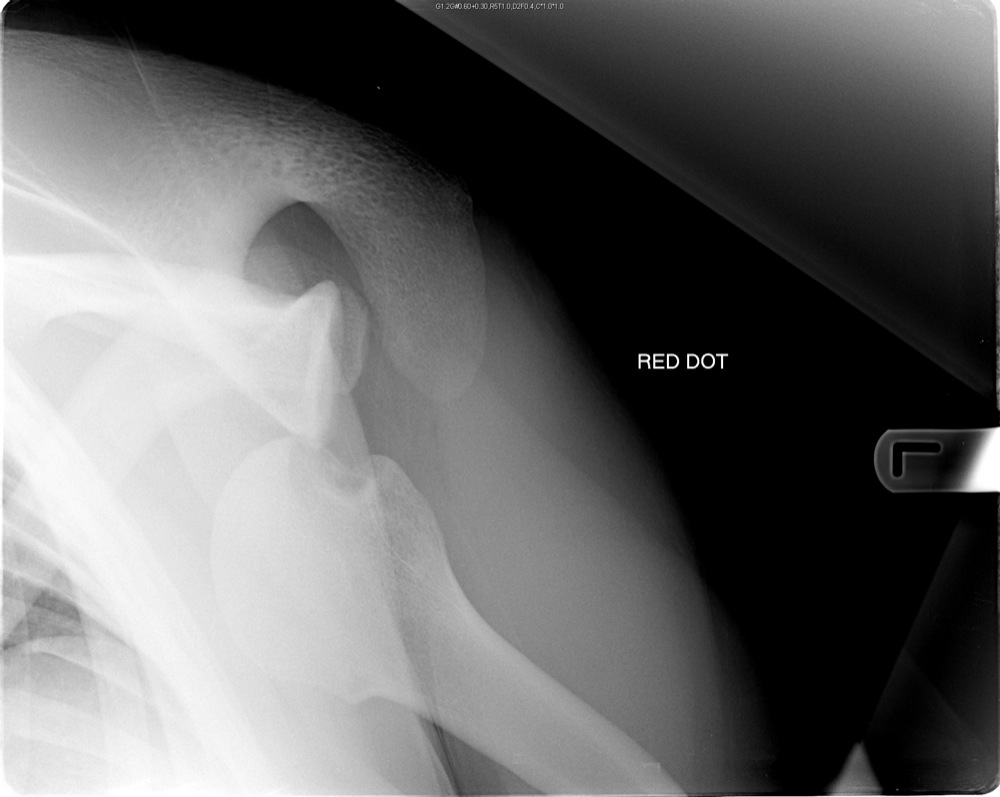
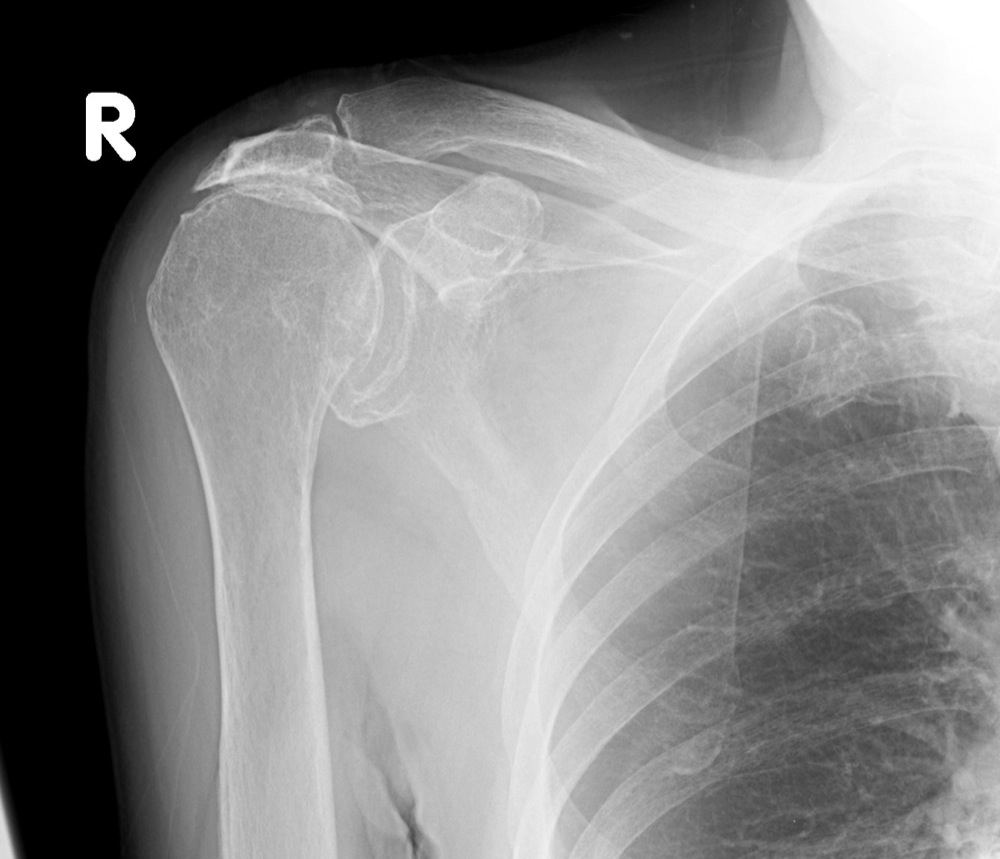
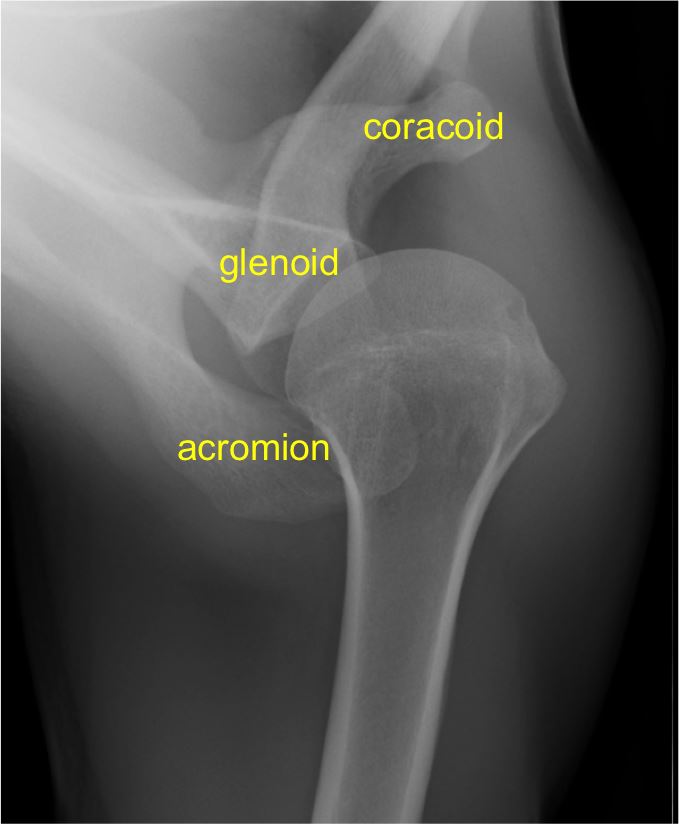
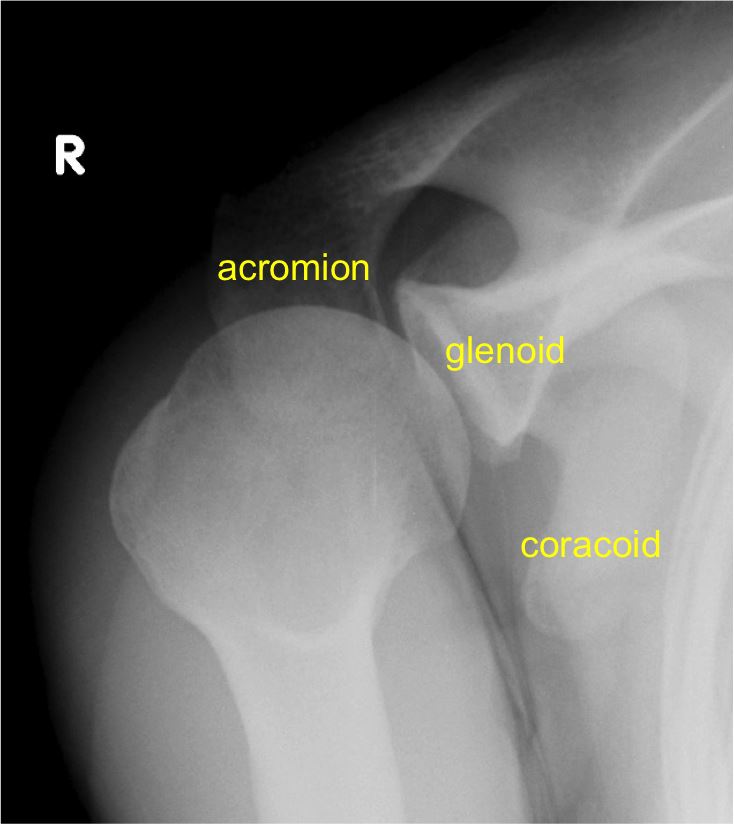
| Glenohumeral joint dislocation | |
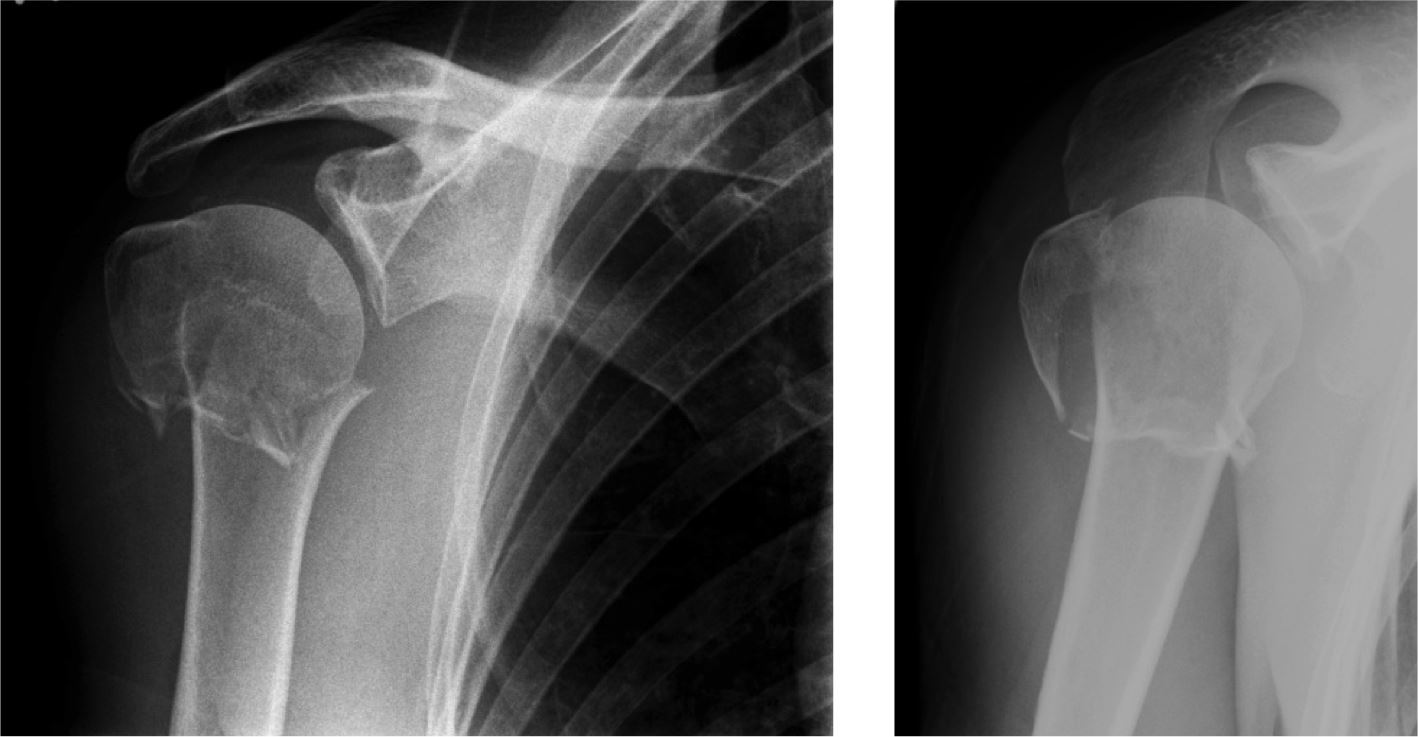
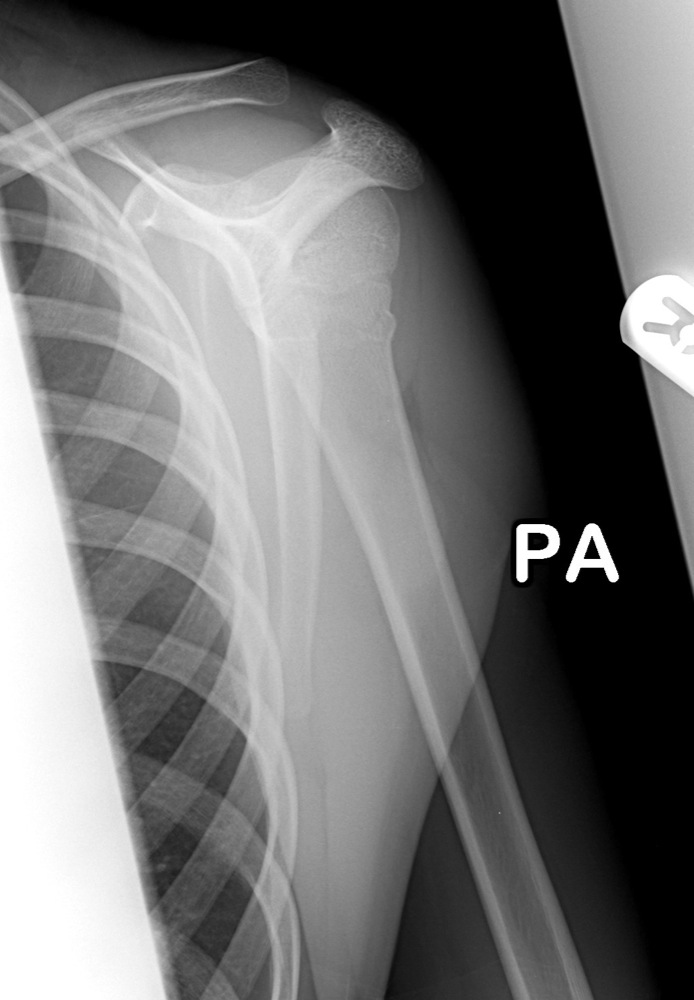
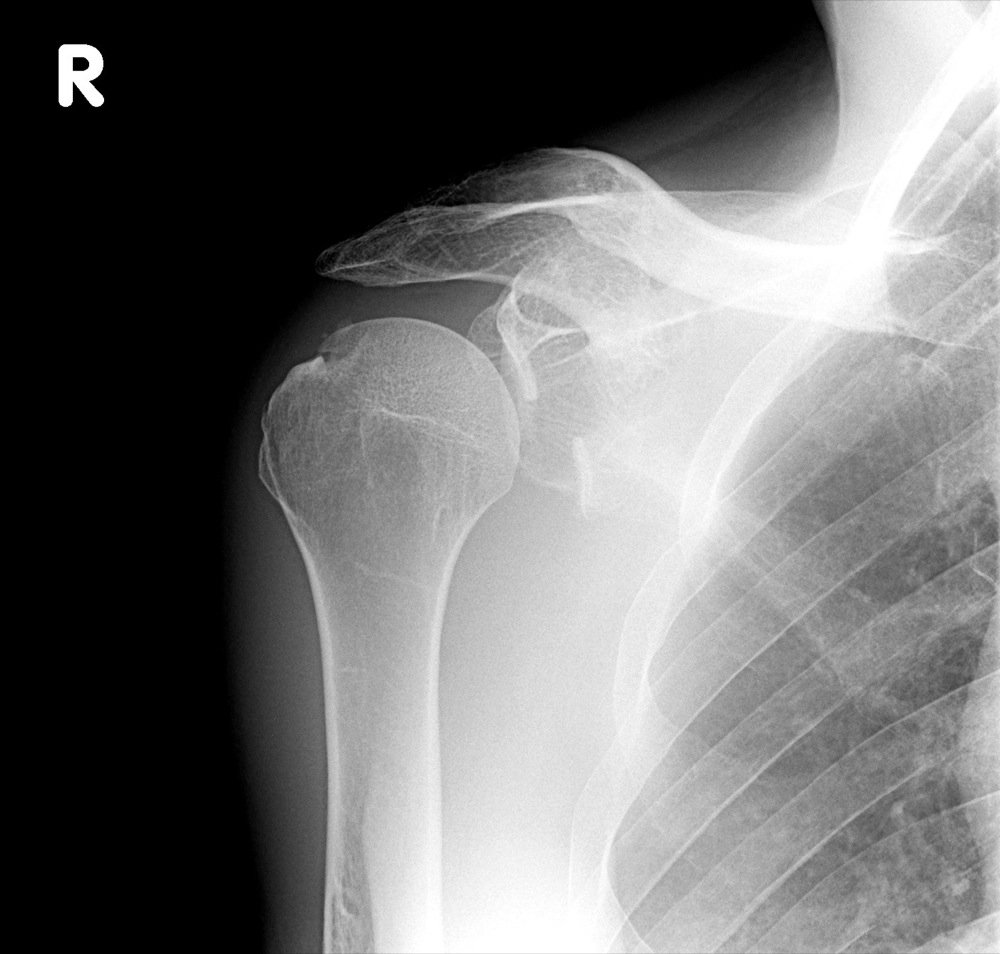
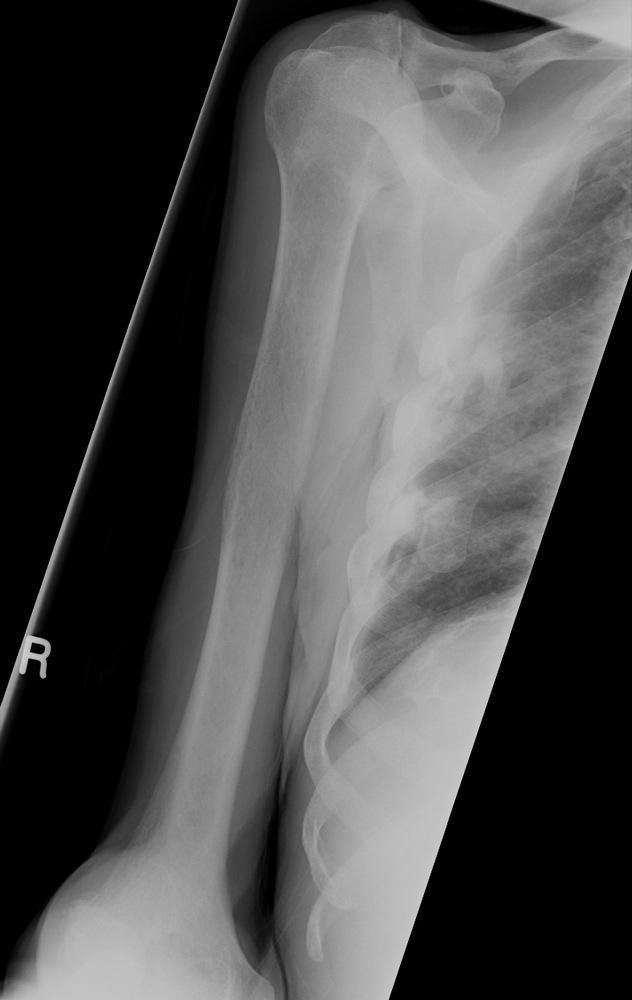
| Under 20 years and over 60 years | Fractured proximal humerus |
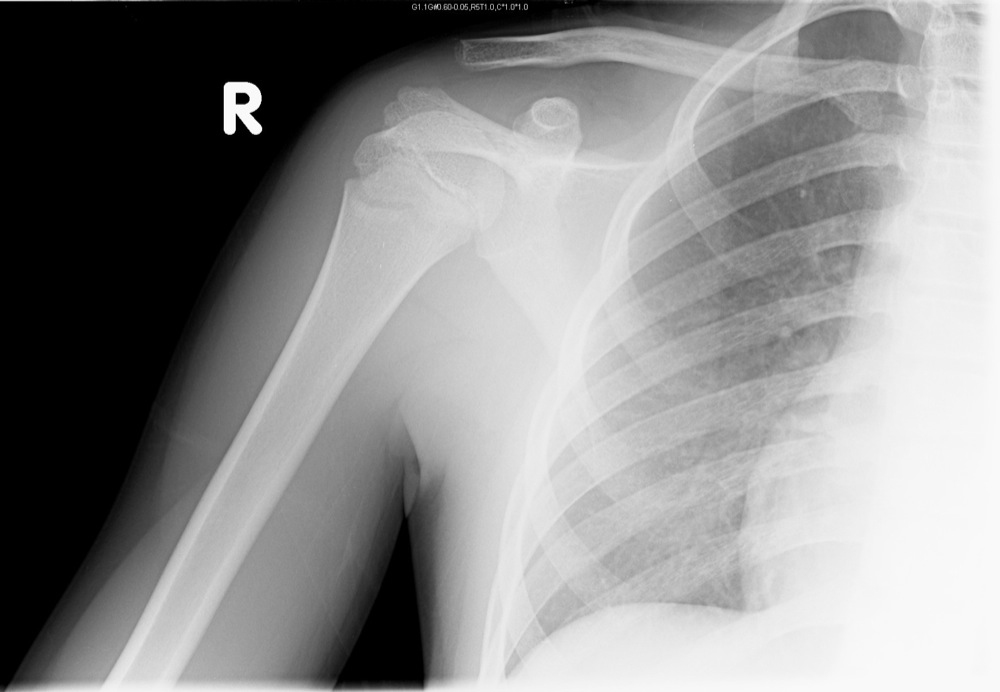
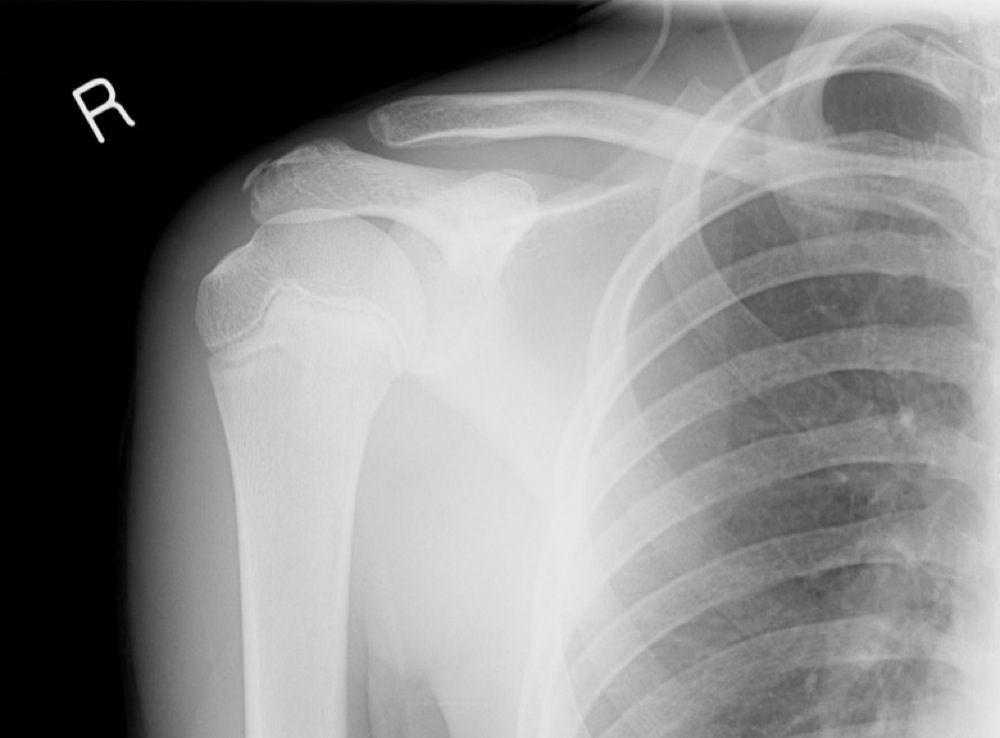
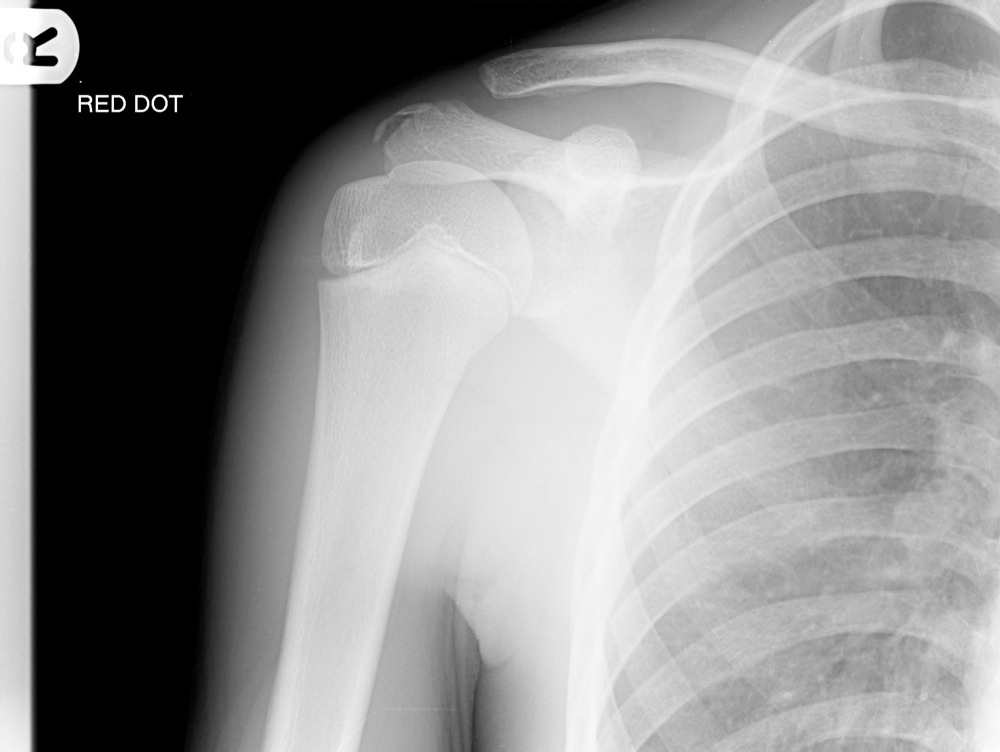


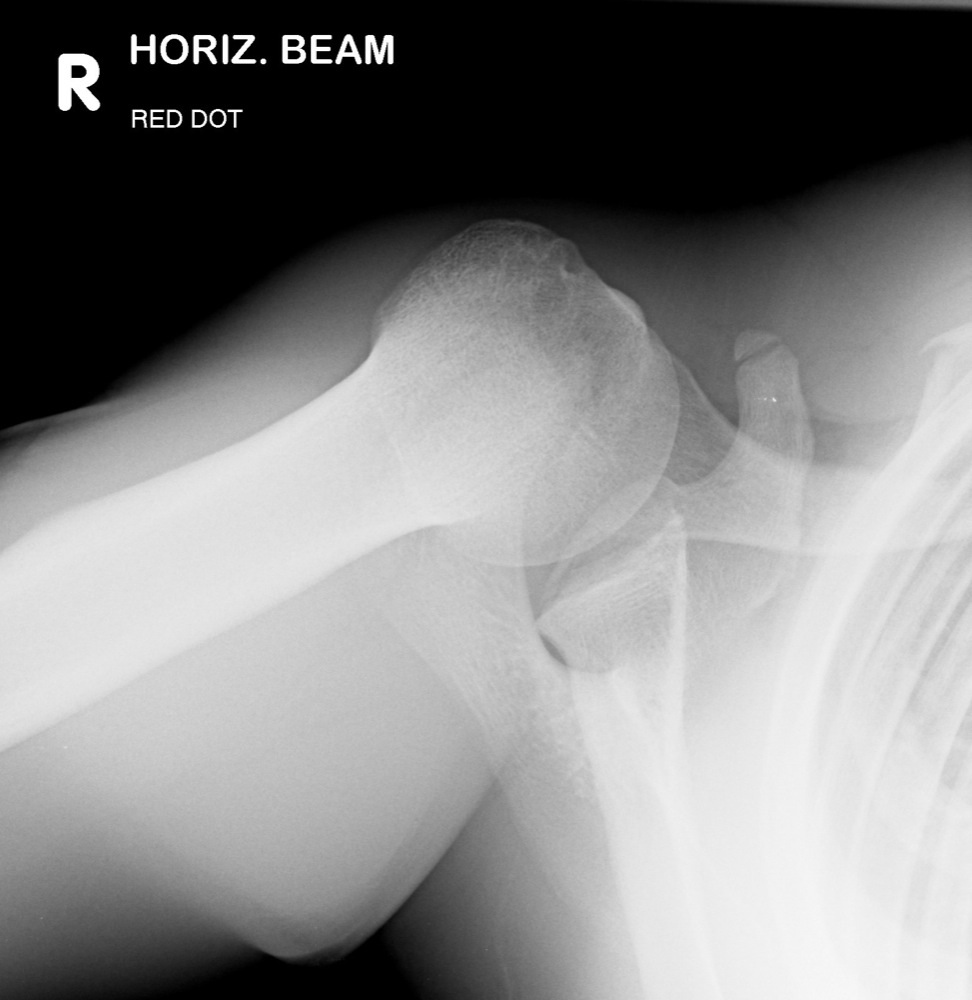
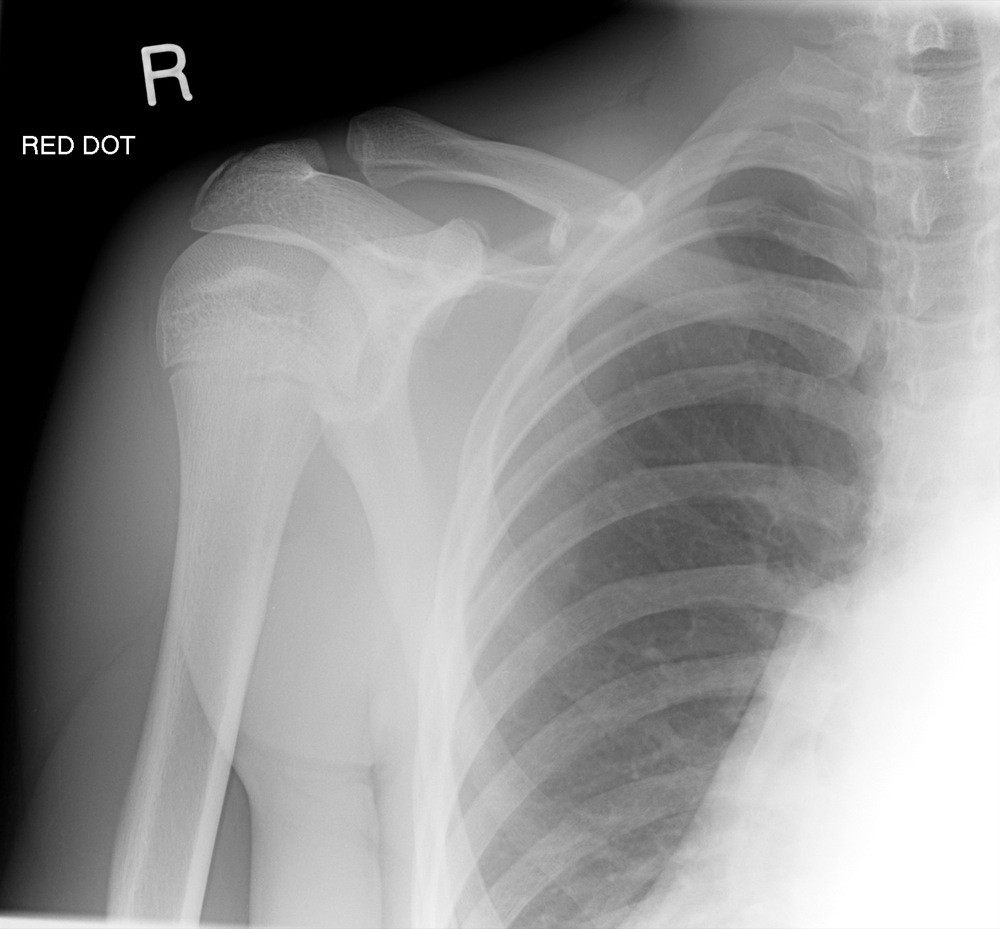
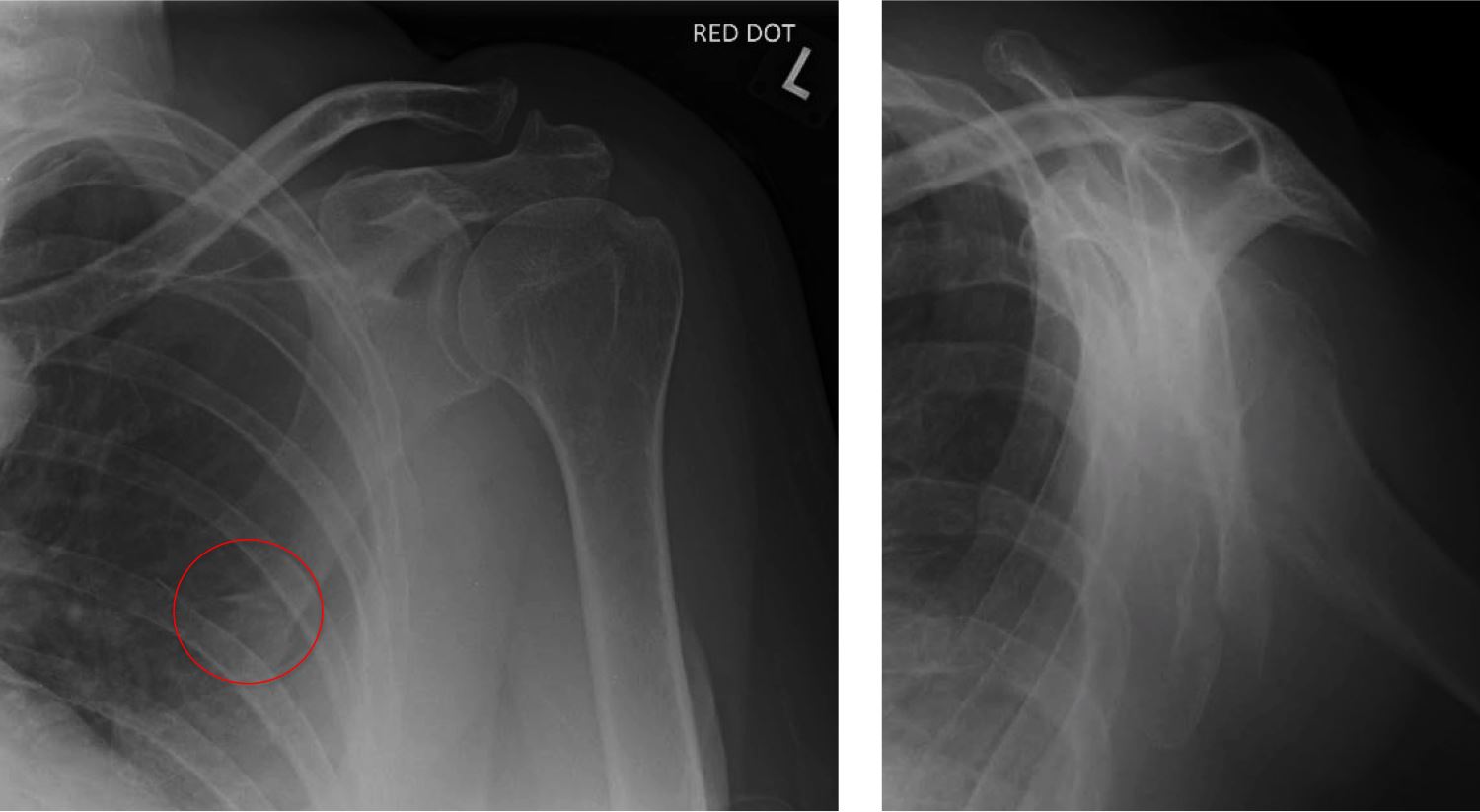
Break to the cortex
Disruption to the trabecular pattern
Sclerosis, suggesting impaction