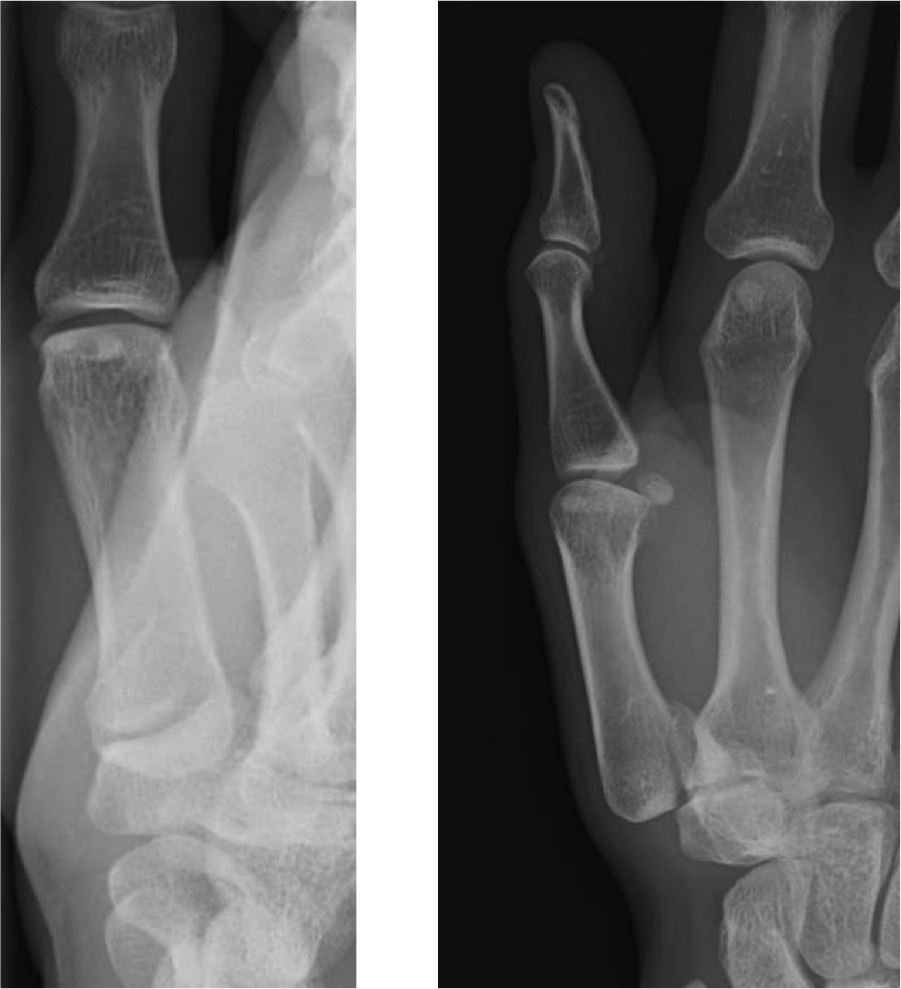
- Fractures to the shaft, neck or head, particularly of the 4th or 5th metacarpal are common. Most often caused by punching injuries. and are rarely missed as they are usually displaced:
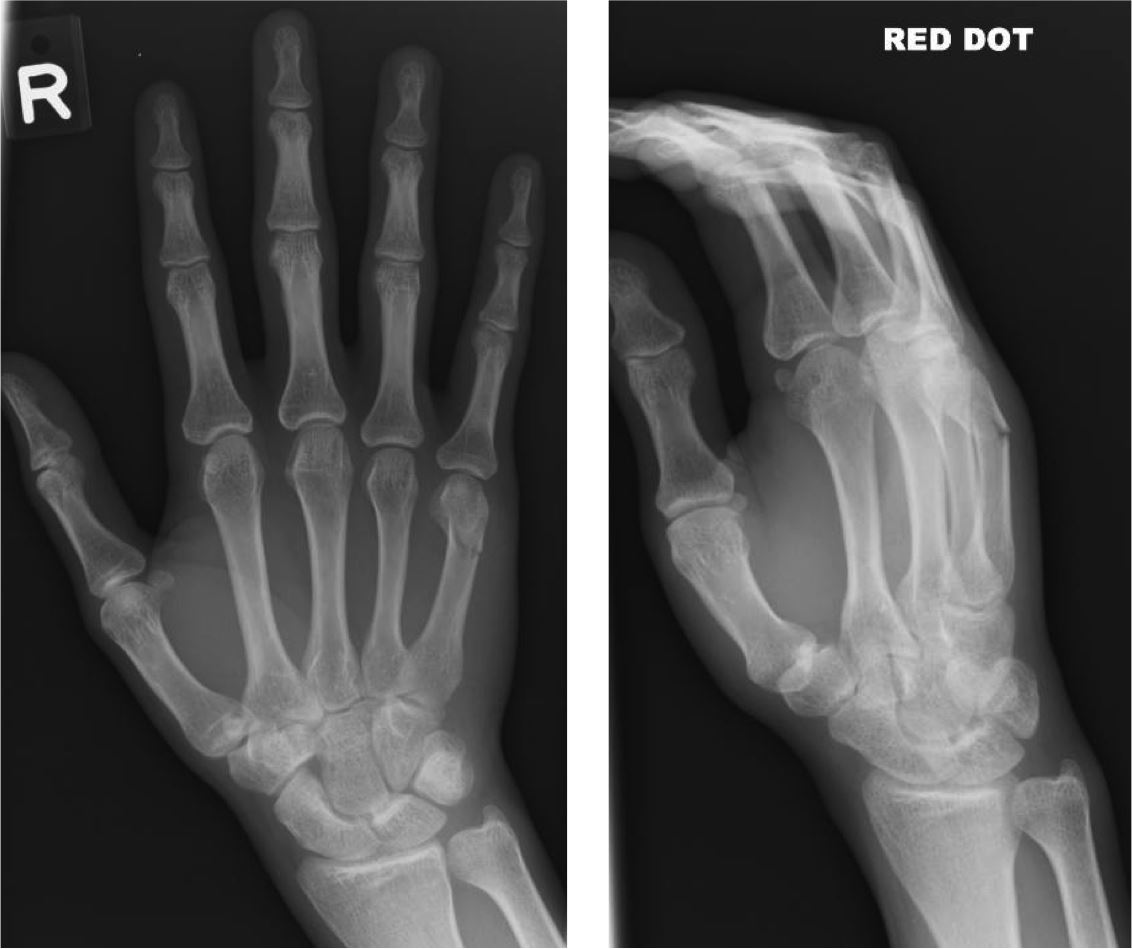
- More subtle, and yet clinically significant, are fractures to the base of the 4th or 5th metacarpal:
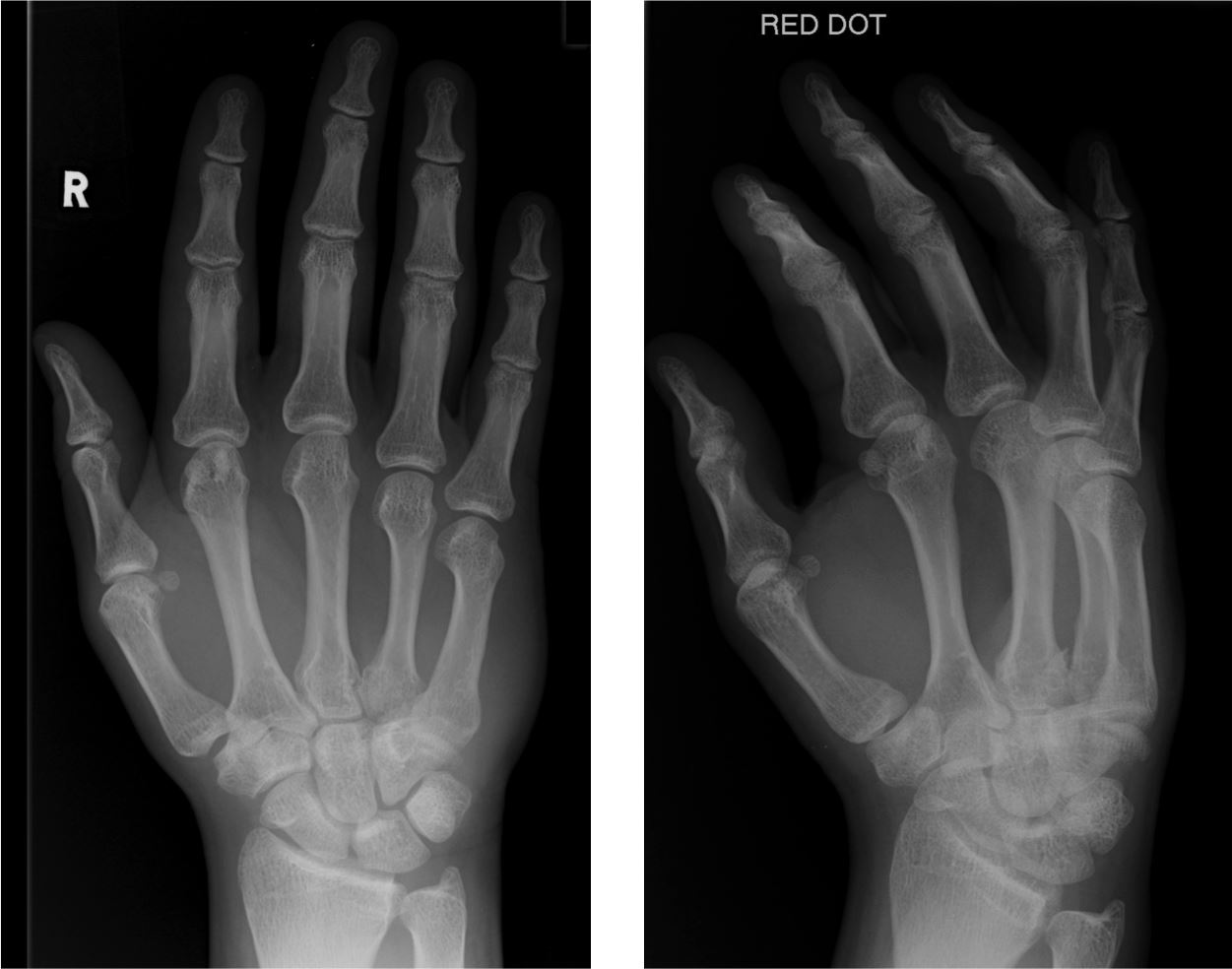
- These are often associated with dislocation to the 4th or 5th carpo-metacarpal joints. A dislocation can be identified by recognising loss of the normal joint space (2mm) at the metacarpal base:
- Another associated injury is to the hamate, often evident on the oblique image:
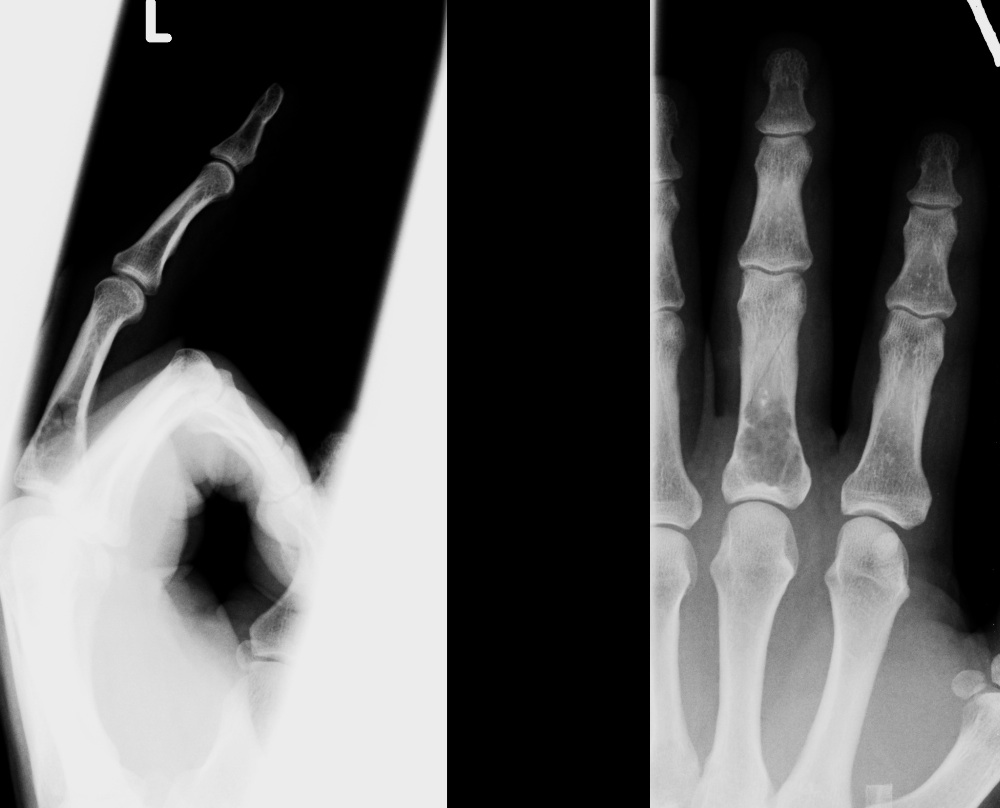
Mechanism of injury is similar to the 5th metacarpal neck fracture so, when index of suspicion is high and a fracture to the head or neck isn't present, scrutinise the
base of the 4th and 5th metacarpals, and the adjacent hamate.