A fall on the out-stretched hand (FOOSH) tends to result in specific injuries depending on the general age of the patient:
- 4-10 years - Torus fracture of the distal radial metaphysis
- 11-16 years - Salter-Harris II fracture involving the physeal plate
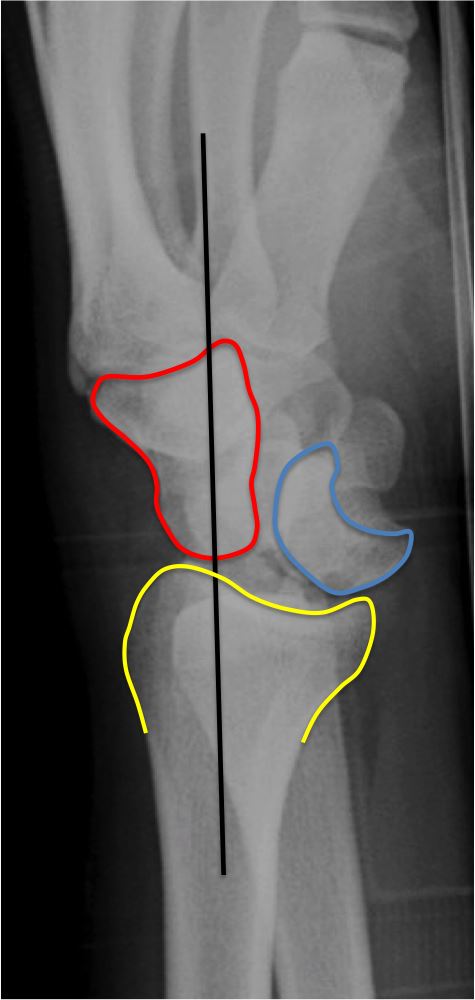
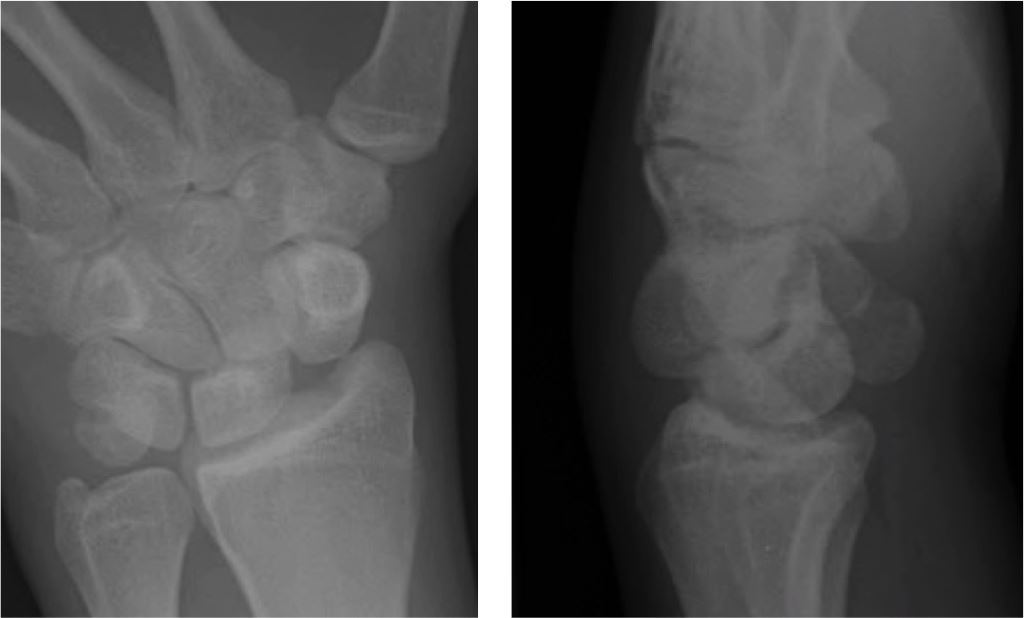
- 17-40 years - Scaphoid fracture
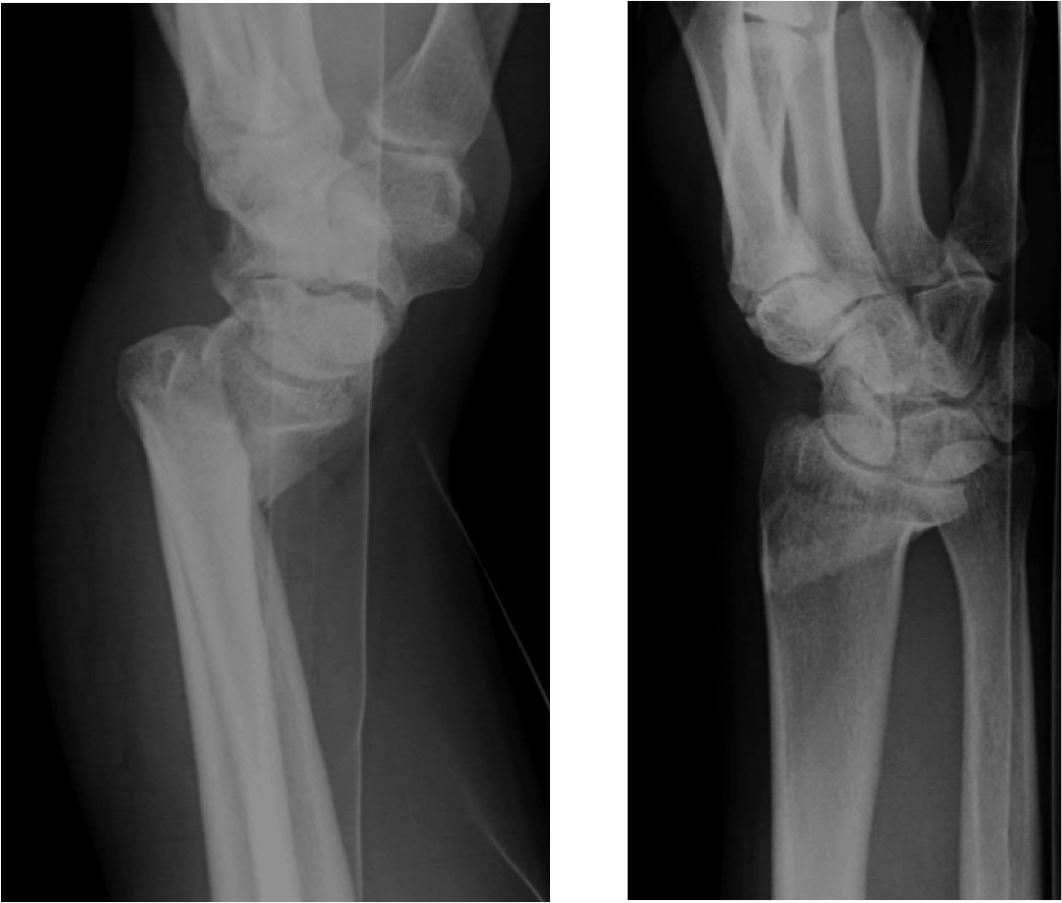
- Over 40 years - Colles'-type fracture