State that a knee radiograph is only required for patients with knee injuries with any of the following:
- Age 55 or over.
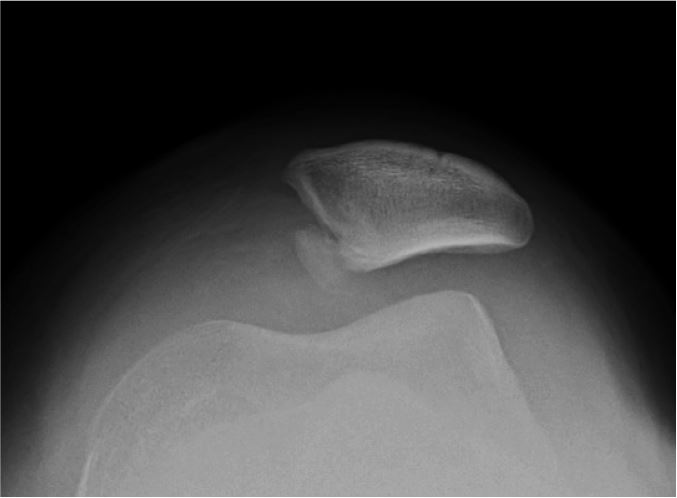
- Isolated tenderness of the patella (no bone tenderness of the knee other than the patella).
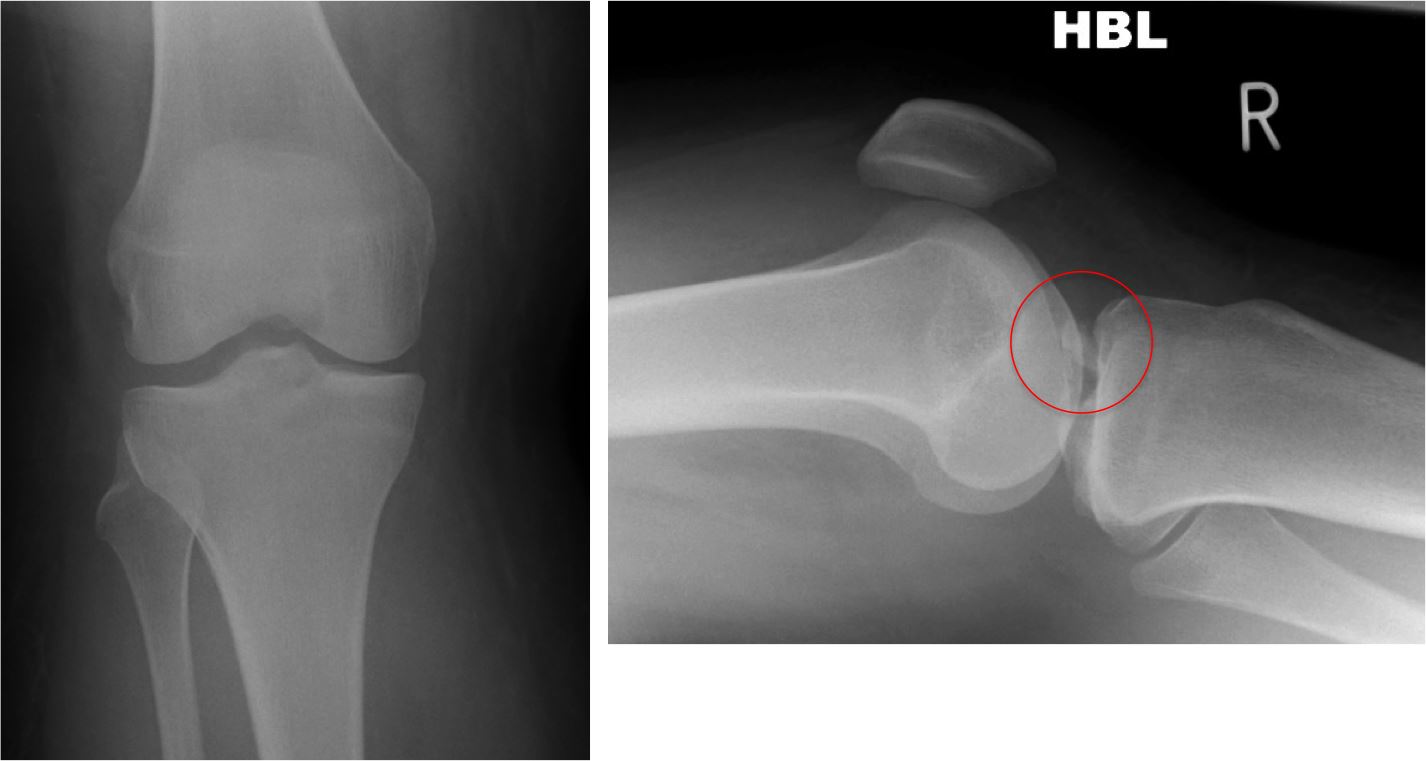
- Tenderness at the head of the fibula.
- Inability to flex to 90 degrees.
- Inability to weight bear both immediately and in the casualty department (ie, 4 steps - unable to transfer weight twice onto each lower limb regardless of limping).